EMR development has changed materially since FHIR became mandatory but many fundamentals stay constant. Understanding both dimensions shapes 2026 development planning.
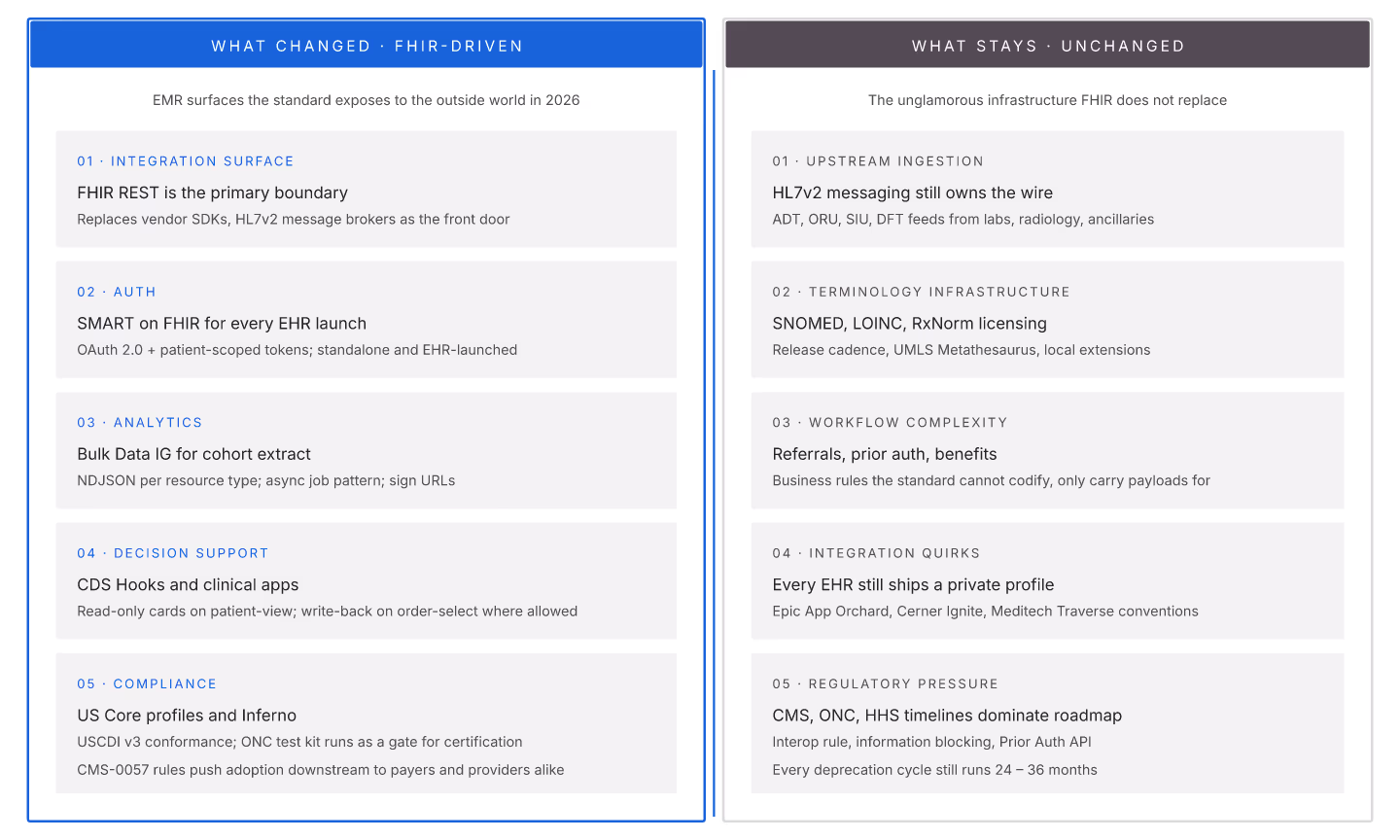
What changed (FHIR-driven)
1. Integration surface = FHIR REST. Custom APIs are legacy; FHIR REST is the ecosystem. 2. Auth = SMART. SMART on FHIR is universal. 3. Analytics = bulk data. Bulk Data IG drives warehouse pipelines. 4. Decision support = CDS Hooks. CDS Hooks fires point-of-care alerts. 5. Compliance = US Core + Inferno. US Core profiles + Inferno verification.
What stays
1. HL7v2 ingestion. Most upstream data is still HL7v2. FHIR complements, doesn't replace. 2. Terminology infrastructure. SNOMED CT, LOINC, RxNorm still dominate. 3. Workflow complexity. Care coordination, referrals, prior auth still complex. 4. Interoperability challenges. Different EHRs, different profiles, different quirks. 5. Regulatory pressure. CMS, ONC still driving requirements.
Development priorities that shifted
| Priority | 2020 | 2026 |
|---|---|---|
| Custom API design | High | Low |
| SMART launch investment | Low | High |
| Terminology server | Optional | Required |
| Bulk data support | Optional | Required |
| Custom auth | Common | Legacy |
| US Core conformance | Nice-to-have | Table stakes |
Development priorities that stayed
1. HL7v2 handling. 2. Terminology governance. 3. Data quality metrics. 4. Backup and recovery. 5. Multi-tenant isolation.
Team skills mix (mid-2026)
1. FHIR spec fluency (up from optional to required). 2. SMART auth knowledge. 3. Terminology domain understanding. 4. HL7v2 (still needed). 5. General software engineering.
EMR development in 2026 is FHIR-first but not FHIR-only. Teams that balance new FHIR skills with retained fundamentals ship better.